





抽象
年龄显著确定COVID-19的临床特征及预后。T型he prognosis was worse in patients older than 60 years, calling for clinicians to pay more attention to patients of this age.https://bit.ly/34DTI05
致编辑:
冠状病毒病2019(COVID-19)的迅速爆发一直是国际关注的疾病的问题正在迅速蔓延[1个,2个]. 考虑到传染病已经在全球范围内造成了巨大的影响,迫切需要确定预后不良的危险人群。在肺部感染期间,衰老与肺部生理、病理和功能的某些变化有关。因此,与年龄相关的反应性和耐受性差异变得明显,导致老年人的临床结局更糟[三]。以前的研究已经提到的,年长的COVID-19的患者死亡的风险增加[4个–7个]。然而,与年龄相关的临床特点,病程和预后比COVID,19例患者死亡等仍不清楚。
总共221谁被诊断由定点医院的发热门诊COVID,19例患者纳入本研究。他们被行政考入上海公共卫生临床中心(上海,中国),以接受医疗服务。诊断是基于病毒核酸检测的积极响应,根据对COVID-19肺炎由中国国家卫生委员会[颁布的诊断和治疗指南的更新版本八]. 本研究分析人口统计学、症状、疾病严重程度及病程、影像学及实验室检查等资料。我们的研究设定了一个统一的观测终点日期(2020年3月7日)。比较两个年龄组COVID-19患者的主要病程转归和继发呼吸衰竭率。
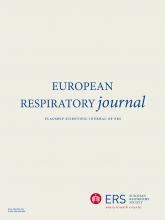
All 221 COVID-19 patients were divided into two groups, taking age 60 years as the threshold. The age distribution for all patients is shown in图1a.136个cases (61.5%) were aged <60 years and the other cases were aged ≥60 years. In total, 176 patients (79.6%) had fever. Other common symptoms included cough (48.0%), sputum (25.8%), sore throat (8.6%) and diarrhoea (5.4%), among which only sore throat showed a significant difference between the two groups (11.8%与3.5%;p值= 0.034)。Significant negative correlations between age of patients and lymphocyte counts (r= −0.432, p<0.001) as well as albumin levels (r= −0.569, p<0.001) were observed in our study (图1b和c)。C类ompared with the younger group, patients aged ≥60 years presented with higher levels of blood urea nitrogen (5.83与4个。4个2个 mmol·L-1个;p<0.001),乳酸脱氢酶(272.8与2个4个9个。0 U·L-1个;p=0.004)和炎症指标(图1d;所有的p <0.01)。In those aged ≥60 years, more lobes were involved (4.15与3.34;P <0.001)在双侧病变(89.4%与74.3%;P = 0.006)(图1e)及患者的比例较高表明细菌共同感染(12.9%与4.4%;P = 0.021)。T型he severity of COVID-19 was milder in those aged <60 years; this younger group showed lower proportions of severe and critical patients (图1f)。In turn, the utilisation of antibiotic therapy, intravenous corticosteroids and assisted ventilation was more common in those aged ≥60 years (图1g)。一onger disease courses and a higher proportion of cases with respiratory failure were observed in patients aged ≥60 years (图1h)。T型he median time of disease course was significantly longer in patients aged ≥60 years (24.0与21.5 天;p=0.026)(图1)。有趣的是,这种差异在男性患者明显显著(25.0与2个1个。0 days; p=0.036) but not in female patients (图1j以及k)。两个年龄组之间,在病程的中位数时间的巨大差异,在合并呼吸衰竭的情况下,虽然显示无统计学意义(38.0与30.0 天;p=0.100)(图1l)。
COVID-19在<60岁和≥60 岁两个年龄组的临床特征和预后的比较。a) 上海市221例COVID-19患者的年龄分布。研究患者年龄与b)淋巴细胞计数(r=-0.432,p<0.001)、c)白蛋白水平(r=-0.569,p<0.001)、d)c-反应蛋白(CRP)水平和血沉(ESR)及e)放射性肺叶的相关性。f)疾病严重程度的差异(根据中国国家卫生委员会的指南,分为轻度、普通、严重或严重[八],但没有轻症病人在我们的队列),G)的治疗,和h)病程,并在两个年龄组的呼吸衰竭率进行了研究。COVID-19的治愈率显示了我)所有的221例患者,j)的男性,k)的女性和L)同呼吸衰竭。*:P <0.05;**:P <0.01;***:P <0.001。
这是第一次系统地评价了年龄对临床特征和重要的成果为COVID-19患者的影响,从而帮助医生建立COVID,19例患者的危险分层尽早。零星有研究指出,老年人可能倾向于感染后死亡[5个,7个,9个],呼吁市民要多加注意保护老人免受病毒。在这项研究中,我们证明了临床特征和221 COVID,19例患者的预后密切相关的不同年龄组。这项研究提供疾病严重程度与年龄之间的关系,这是其他研究没有明确的证据。这些指标综合分析将提供全球范围内的医生与疾病认知,状态评估和有效的治疗COVID-19的重要信息。
T型he proportion of patients using antibiotics was higher in patients aged ≥60 years than in patients aged <60 years, possibly due to the higher proportion of patients with bacterial co-infection in this group. Besides, older patients showed more serious illness, leading to higher frequency of adjuvant therapies including corticosteroids and assisted ventilation in this group of patients. Consistent with recent reports [10,11],年龄较大的患者呈现淋巴细胞比年轻患者的显著较低水平。淋巴细胞一般被升高响应于常见病毒感染,但在严重急性呼吸综合征(SARS)和COVID-19 [被异常降低12–14]. 尽管其机制尚不清楚,但低水平的淋巴细胞可能是COVID-19疾病严重程度的一个关键指标。其他血清学指标,如白蛋白、血尿素氮、乳酸脱氢酶、炎症指标等,也随着年龄的增长而呈上升趋势。这一现象是显而易见的;然而,我们无法确定这些变化的指标是否导致或导致疾病严重程度随年龄的差异。
虽然大多数患者在这项研究中具有良好的预后,有些患者需要治疗,这可能已经变成了糟糕的时间较长,由于医院获得性或医源性感染的高风险。年龄在病毒感染研究危险因素疾病严重程度和死亡的一个[5个,9个],尽管有关年龄在这些研究中的数据是近似的。Our study found that COVID-19 patients aged ≥60 years had a higher rate of respiratory failure and needed more prolonged treatment than those aged <60 years, demonstrating that elderly COVID-19 patients had much more severe disease and showed poorer response to treatments than the younger age group. The cure rate of patients aged ≥60 years (89.4%) was relatively lower than that of patients aged <60 years (95.6%), especially in males and those with respiratory failure. A previous study indicated that there might be a sex predisposition to COVID-19, with men more prone to be affected, but gave no evidence of an association between the severity of COVID-19 and the male sex [15]。需要更多地注意支付给这些老年患者呼吸衰竭,积极的早期干预提出,要改善他们的预后。随着来自不同种族和遗传背景的被检查更多的情况下,在这项研究中与年龄有关,这一发现可能由医师全世界得到证实。
总之,临床特点和疾病的预后不同年龄段的患者中变化和年龄进行全面评估可以帮助全球医生建立风险分层所有COVID-19例。Patients aged ≥60 years showed heavier clinical manifestations, greater severity and longer disease courses compared with those aged <60 years. Closer monitoring and more medical interventions may be needed for the elderly.
可共享的PDF
致谢
作者想表达诚挚的感谢所有的医院,也给患者的这项研究贡献的所有人员。
脚注
作者贡献:徐金福、曲洁明对本研究进行了构思和设计。刘洋、毛蓓、梁朔、陆海文、柴燕华、徐金富进行了初步分析,并准备了初稿。王岚、张莉、李秋红、赵岚、何彦、顾小龙、季小斌、李莉、李志军、李强、李向阳、卢洪周、张文红、宋元林对选稿进行了智力内容的审查。通讯作者徐金富、曲洁明对研究中的所有数据都有充分的访问权,并对数据的完整性和数据分析的准确性负责。
利益冲突:刘洋有没有透露。
利益冲突:北毛有没有透露。
利益冲突:硕良有没有透露。
利益冲突:佳威扬有没有透露。
利益冲突:陆海文无需透露。
利益冲突:闫华柴智屏没有透露。
利益冲突:兰望有没有透露。
利益冲突:李章有没有透露。
利益冲突:邱虹立有没有透露。
利益冲突:拦着有没有透露。
利益冲突:何燕有没有透露。
利益冲突:小龙顾无需透露。
利益冲突:肖彬纪有没有透露。
利益冲突:李莉有没有透露。
利益冲突:志骏捷有没有透露。
利益冲突:李强有没有透露。
利益冲突:向阳力无需透露。
利益冲突:洪周璐无需透露。
利益冲突:文张鸿有没有透露。
利益冲突:袁林嵩有没有透露。
利益冲突:节明曲有没有透露。
利益冲突:徐金富无需透露。
支持声明:该作品得到了国家自然科学基金杰出青年学者到金赋序(81925001),上海领军人才计划(编号2016036至金赋序)和上海医院发展中心的项目(16CR3036A支持以金赋序)。该资助者在设计和研究的行为没有任何作用;收集,管理,分析和解释数据;审查或手稿的批准;并决定提交书稿出版。没有作者已支付的任何制药公司或机构来写这篇文章。本文资金的信息已交存交叉引用出资者注册.
- 收到二〇二〇年三月二十〇日。
- 认可的2020年4月11日。
- 版权所有©ERS 2020
本版本根据知识共享署名非商业许可4.0条款分发。







![Comparison of clinical features and outcomes of COVID-19 between two age groups, <60 and ≥60 years. a) Age distribution for all 221 COVID-19 patients in Shanghai. Correlations were investigated between the age of patients and b) lymphocyte count (r= −0.432, p<0.001), c) albumin level (r= −0.569, p<0.001), d) C-reactive protein (CRP) level and erythrocyte sedimentation rate (ESR), and e) radiologically affected lobes. The difference in f) disease severity (classified as mild, common, severe or critical, according to the guidelines from the National Health Commission of China [8], but with no mild patients in our cohort), g) treatment, and h) disease course and rate of respiratory failure in the two age groups were also investigated. Cure rates of COVID-19 are shown for i) all 221 patients, j) males, k) females and l) those with respiratory failure. *: p<0.05; **: p<0.01; ***: p<0.001.](http://www.qdcxjkg.com/content/erj/55/5/2001112/F1.large.jpg?width=800&height=600&carousel=1){kind=link}
{kind=link}